NEW COLUMN is “Kung Flu Is A Killer, All Right, But So Are The Bureaucrats.” It is currently on WND.COM and the Unz Review.
Excerpt:
“When, Mr. President, will you deliver instant, standardized, country-wide testing to all the American people,” comes the daily, petulant demand from the malfunctioning media, reiterated by the expert class and an intelligentsia that is not always very intelligent.
The hype over testing will be the next contagion of illogic on matters related to coronavirus.
The testy twits are treating COVID testing as though it were an amulet against the dreaded disease. It isn’t. All testing does is give an individual a snapshot in time of his COVID status. As soon as he drives out of the testing facility, a COVID-free person could become infected.
Unless they engage in prevention, a single testing in time doesn’t in any way give individuals a clean bill of health.
Prevention protects people.
Testing is, however—at this stage of spread—helpful in giving medical researchers a grip on the symptomless-sick phenomenon, as well as an idea of how the disease is disseminated and distributed in the population.
Test and keep testing large enough representative samples, and you’ll get good prevalence data. You’ll probably discover statistically significant differences in COVID infection rates along the rural/metropolitan axis, and the Chinese/no-Chinese axis.
In fact, high-tech meccas are likely a good proxy for the correlation between COVID and the Chinese population. Hubs of high-tech like my state of Washington—the King and Snohomish counties, in particular—have high coronavirus infection rates.
Antibody status is another essential parameter obtained from testing. In addition to identifying the prevalence of disease in the population, a COVID serology assay will divulge who has developed antibodies to the virus, is now immune to it, and can get on with it.
But unless you vigorously protect your health status with barriers to SARS-CoV-2, testing is but a snapshot in time of your disease status.
In the fullness of time, mainstream will arrive at these simple deductions.
Before the testing fetish came the face-mask mythology. Face masks were the first contagion of illogic sprung on a gullible public.
Most “covidiots” insisted that, because the “experts” had said so, donning face masks during an epidemic to reduce droplet transmission was futile. Proven. Q.E.D. Nothing more to show.
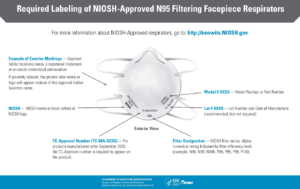
But, as far back as March 5, in “Unmasking Statist, Socialist Propaganda About ‘Face Masks,’” this column unpacked the lies and illogic underlying the contention that masks (surgical and N95) were worthless to the public. As follows:
“While the coronavirus is indeed minuscule, smaller than 0.3 microns (likely between 0.1 and 0.2 microns), COVID-19 is delivered in a larger medium of bodily fluids or spray. Certainly, some barrier to the spittle in which the coronavirus is dispersed is better than none.”
“No surprise then, that world health authorities can’t seem to get their story straight on masks. At times, they concede ‘that N-95 face masks are protective.’ More frequently, they scratch the proverbial proboscis (ostensibly a sign of lying) and say ‘No, of course, they’re ineffective.’ In other words, ‘they work for me, the healthcare worker, but not for thee.’”
“For honesty’s sake,” I had exhorted, “the country’s health-care functionaries might appeal to consumers on the ground of dire shortages. But on the basis that no protection is better than some protection? Please! …”
On March 30, our great Tucker Carlson seconded my mask message of March 5, emphasizing the arguments above. Two days prior to Tucker, 23 days after Mercer—a lifetime in a pandemic—mainstream caught up. Wrote the New York Post: “Experts say face masks can help slow COVID-19, despite previous claims.”
A full month after this column’s advice to ignore government enjoinders against face masks and respirators, the government has reversed its position.
On April 3, government grandees finally instructed Americans to cover their faces with anything but surgical and N95 masks. In so doing, the government had stopped flouting logic and had come clean about why it had endangered American lives.
As pinpointed in my unmasking of March 5, the depraved calculus that went into advising Americans initially, and unintuitively, not to shield viral entry points—mouth, eyes and nose—was purely utilitarian. It stemmed from a fear that, by protecting their health, citizens would contribute to scarcity and undermine the health of healthcare workers.
Sold to the public as settled science, the initial mask fallacy-disguised-as-policy was social engineering for the sake of resource conservation. …
… READ THE REST. NEW COLUMN is “Kung Flu Is A Killer, All Right, But So Are The Bureaucrats.” It is currently on WND.COM and the Unz Review.
* Image is of Hydroxychloroquine Via AP



 I try to tell people
I try to tell people