Tucker Carlson is the only man in mainstream conservative media to be standing “athwart history, yelling ‘Stop,’ at a time when no one is inclined to do so, or to have much patience with those who so urge it.” (The rest on Fox News should be screened out as so much white noise.)
And Mr. Carlson has cobbled together convincing anecdotes to support his assertion that race will increasingly determine which patient gets critical Covid treatment. In particular, in an existing “equity” based point-system, a patient gets no points for being … white.
Pockets of free-market medicine once enjoyed might have remedied this. But these are clearly drying up due to a tight collusion between the constituent elements of the Pharma State, working to centralize the dispensing of Covid therapeutics, so as to wield scarcity as a political weapon in bringing about compliance.
As to Carlson’s question, “Why are Americans putting up with this?”: That’s more than a bit cynical, sir.
The answer: Most Americans are in denial about the systemically anti-white nature of their society. Too many are in a twisted a state of torpor, too stupid to do anything but turn their wrath on the unvaccinated—sicced like dogs on their neighbors, rather than on the Pharma State.
Above all, “When you aren’t a celebrity host, sir, your power is limited—and your advocates, the GOP, are busy advocating for war in East Europe, aid to Afghanistan, lower taxes, blah, blah.” Get it?
Several weeks ago, for example, the Food and Drug Administration released a factsheet on a monoclonal antibody called sotrovimab.
Sotrovimab is at this point, the only monoclonal antibody treatment that is proven effective against the latest variant of the coronavirus. The F.D.A. provided guidance for physicians in all 50 states telling them how to determine which patients should get this treatment, this critical treatment.
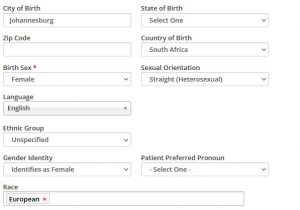
Physicians, the F.D.A. explained should consider quote, “race and ethnicity” as they administer treatments and so physicians are doing that across the country.
In Utah, COVID patients are triaged by a scoring system that determines whether or not they qualify for these potentially lifesaving antibody treatments. Look at this chart, it shows the scoring system. You’ll notice that race often counts more than physical health.
The State of Utah, for example, gives two points to anyone simply for not being white. You win if you’re not white. If you have congestive heart failure at the same time, you get one point. So if you’re a white congestive heart failure patient, that’s not enough for you.
It’s the same story in Minnesota. Minnesota awards two points to so-called BIPOC patients. That means anyone who is not white. If you have high blood pressure and you’re 60 years old, you get one point. So tough luck for you. Imagine if that was one of your parents. It is one of someone’s parents.
In New York, writes Aaron Sibarium, in a shocking new piece for “The Washington Free Beacon,” quote, “Racial minorities are automatically eligible for scarce COVID-19 therapeutics, regardless of age or underlying conditions.” It doesn’t matter what kind of health they’re in, all that matters is their skin color. Whites don’t qualify.
This is not healthcare, its punishment. It is punishment meted out on the basis of skin color.
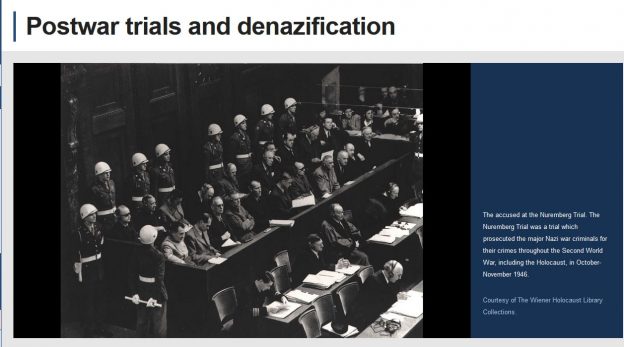
Now, the justification for all of this, the authorities could not be clearer about it. They’ve taken their ideas directly from America’s colleges, they will tell you why they’re doing this. The justification is history.
The United States has mistreated racial minorities in centuries past, they say, therefore, whites must suffer now. So your ancestors did bad things or people who looked like your ancestors did bad things, so now, we are withholding medicine from you.
They call this equity. It’s not equity. It is collective punishment. It’s the North Korean standard. It’s the definition of evil.
And in case you’re wondering if that’s actually what it is, consider this. A young Haitian man could cross our border illegally today, many have. That person could show up at a clinic in New York tomorrow for COVID treatment, and get preference over an elderly American citizen purely because of his appearance.
Think about that. The Haitian has not suffered from systemic racism in America, whatever that is, he just got here. But he goes to the front of the line anyway. Now, that’s not a criticism of the Haitian, it is not his fault. He didn’t make the rules.
But the Americans who did make the rules clearly didn’t make them on the basis of public health. They made them in an effort to hurt a specific group of Americans and they are succeeding. This is happening everywhere, even in places you would never expect it to happen.
Watch as this man talks to an employee at a Texas medical facility to find out exactly what their policies are.
(BEGIN VIDEO CLIP)
UNIDENTIFIED MALE: So I’m not able to get it today?
UNIDENTIFIED FEMALE: Nuh-uh.
UNIDENTIFIED MALE: Because I don’t qualify.
UNIDENTIFIED FEMALE: Yes.
UNIDENTIFIED MALE: What if I — what if I like smoke and vape? I heard that was okay.
UNIDENTIFIED FEMALE: No.
UNIDENTIFIED MALE: Okay. But if I were black and Hispanic, then I’d be able to qualify. Okay, I’m being denied medical service because of my race, is that —
UNIDENTIFIED FEMALE: That’s the criteria.
(END VIDEO CLIP)
CARLSON: So you can’t get lifesaving drugs from the government of Texas if you’re the wrong color. Think about that.
We reached out to the Texas Department of Health about this back in November and they denied allocating any healthcare on the basis of race, but of course they were lying. The North Central Texas COVID-19 Regional Infusion Center was created by the Texas Department of Health.
Last year, the Infusion Center’s website which says it is state funded featured an information sheet that explicitly listed race as an eligibility factor for getting antibody therapy. That’s what you just saw there, someone being denied medical treatment because he is the wrong color, without even assessing the relative health risks involved.
The website maintained by the Tarrant County, Texas — by the County of Tarrant in Texas explains that being nonwhite automatically makes you eligible for treatments. So this is still happening on a wide scale.
The question is, why are Americans putting up with this? It’s immoral. We’re used to hearing that your kids can’t get into a certain school if they are the wrong color or get a certain job if they don’t have the right appearance, and apparently they have accepted that.
UPDATE (1/14/022): “FDA wants race, ethnicity factored in administering COVID drugs” If White, Avoid moving to Utah and Minnesota run by racists:
“Risk factors for hospitalization and mortality are now well-recognized and include age, cumulative comorbidities, male gender, shortness of breath, and importantly, but for reasons not well-understood, non-white race/ethnicity,” read state guidelines on the standards of care of monoclonal antibody treatment.
However, Utah has also provided “ethical justification” for its patient selection.
“Utah Data from more than one hundred thousand patients with COVID-19 confirms that even after controlling for age and comorbidities, Utahns who identify from communities of color have a significantly higher risk of severe disease requiring hospitalization,” the guidelines read. “Public health interventions may be used to attempt to mitigate these disparities in COVID-19 by recognizing the structural inequities that underlie them. One way to do this is to include race/ethnicity in the patient selection criteria.”
Minnesota health officials have also urged health care providers to “consider heightened risk of progression to severe COVID-19 associated with race and ethnicity when determining eligibility” for monoclonal antibody treatment of COVID-19.
UPDATE II (1/17/022):
“Midwest Catholic hospital system says it will cease discrimination against WHITE patients when offering COVID monoclonal antibody treatment after conservative law firm threatened to sue
* Image credit